1. What Are Fibroids?
Fibroids, also known as “myoma” or “leiomyoma”, are muscular growths found in the uterus. They are made up of smooth muscles that develop into a non-functional “tumour” when a single cell overmultiplies.
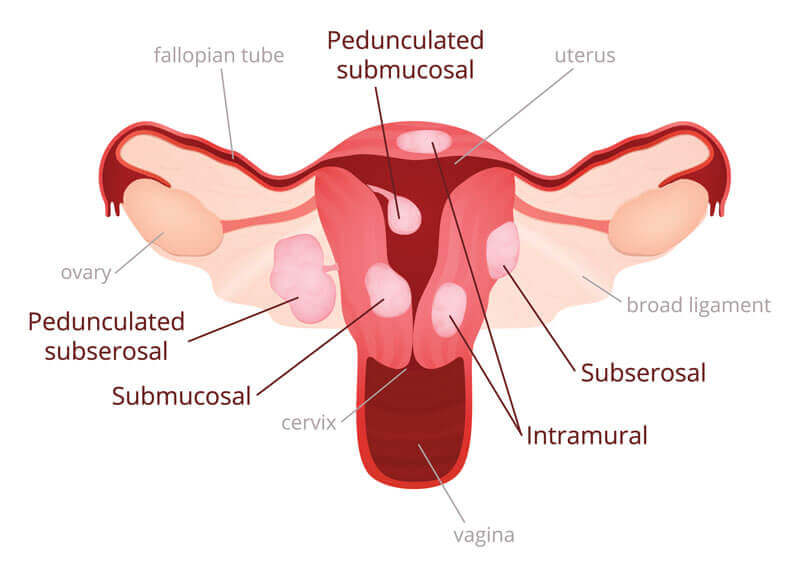
Fibroids vary in size and can be classified into 3 main types.
- Subserosal fibroids: These fibroids form on the outside wall of the uterus and into the pelvis.
- Intramural fibroids: These fibroids form within the wall of the uterus.
- Submucosal fibroids: These fibroids form underneath the uterus inner lining and can grow into the womb cavity, causing complications.
2. How Common Are Fibroids?
Fibroids are very common and are found in up to 30% of all women, especially during the reproductive years (approximately 16 to 50 years old). Many women may not be aware that they have fibroids since only about 1 in 3 women would experience symptoms like heavy or painful periods, abdominal or lower back pain, frequent urination, and pain during sex. Fibroids can be easily diagnosed with an ultrasound scan.
3. Can Fibroids Cause Infertility?
Yes, fibroids can cause infertility in certain instances. This is highly dependent on the position of the fibroids, for example, if the fibroids are displacing the ovaries or blocking the fallopian tubes. Submucosal and deep intramural fibroids also have a higher risk of causing infertility and studies have shown that removal of these types of fibroids can improve pregnancy rates.
4. Do Fibroids Affect Pregnancy?
Fibroids have been associated with the following conditions during pregnancy:
- Miscarriage
- Preterm labour
- Pain in pregnancy due to red degeneration
- Placenta problems
- Breech presentation
- Obstructed labour
The impact on the pregnancy will depend on the size and site of the fibroids. The number of fibroids may also be a factor, but to a lesser extent.
Fibroids during pregnancy can affect:
- Where the pregnancy grows
- Where the placenta implants
- The baby’s position in the womb if the fibroids are sufficiently large
Fibroids may also enlarge rapidly during pregnancy.
5. Should You Remove Fibroids Before Pregnancy?
No, you do not have to remove the fibroids if it is not going to impact pregnancy.
Yes, you should remove the fibroids if it has been proven or anticipated to cause problems in pregnancy.
6. Should You Remove Fibroids During A Caesarean Section?
The standard answer is no but if the fibroid is pedunculated, which means it is attached to the uterus by a thin stalk of tissue, or causing obstruction, exceptions might be made. It is usually not advised because the risk for bleeding is greatly increased due to the increase in blood supply and engorged blood vessels in the pregnant uterus.
7. Can You Have A Normal Delivery After Removing Fibroids?
It depends on the depth and size of the fibroids. If the fibroid was superficial (ie. serosal), and the removal was done via a hysteroscopic procedure, you can still have a normal delivery. However, if a deep intramural fibroid was removed with a deep incision, you may need to discuss with your obstetrician-gynaecologist if you could still have a natural delivery.
8. Can Fibroids Recur or Regrow?
Yes, definitely. The recurrence rate of fibroids is about 30-40%. Predisposing factors include age, race, the number of times the woman has given birth, and the number of fibroids removed. Generally, fibroids are hormonal dependent and there should not be any further growth after a woman reaches menopause.
9. Are There Medications to Treat Fibroids?
GnRHa injections induce a temporary menopause state and have been used to shrink fibroids before surgery. The effect is not long lasting and the fibroids quickly revert to its original size upon cessation of the treatment.
Ulipristal, a selective progestogen receptor modulator, has been shown to be effective in fibroid shrinkage (30-40% volume) and holds the promise for a longer term treatment. It can be repeated up to 4 courses over 18 months and the effects can potentially last longer.
10. Can You Leave Fibroids Alone?
It depends on the clinical scenario. Some small fibroids can cause big problems while some big fibroids are hardly harmful. Regular screenings with your gynaecologist are encouraged for early detection, monitoring, and management of fibroids. Treatment will be based on the anticipation and clinical assessment of the patient.